|
|
|
Anterior Cruciate Ligament Rupture(Reprinted by permission from pamphlet distributed by the Southern California Surgical Group of Irvine, California) The Athletic Rear Limb LamenessThe most common cause of rear limb lameness in the dog is rupture of the anterior cruciate ligament. This injury allows degenerative changes to occur in the stifle (knee) joint which must be limited before permanent cartilage and bony changes occur and result in irreversible arthritis.
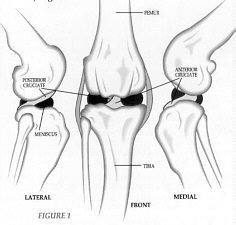
The stifle is a hinge joint which allows a wide range of motion of the tibia on the
femur. To maintain stability through this range of motion there are two cruciate
ligaments, one anterior (toward the front of the knee) and one posterior. These ligaments
cross each other (hence the name cruciate) to provide a major role in stifle stability.
The anterior cruciate ligament also prevents forward displacement of the tibia on the
femur (anterior drawer motion). Fig. 1.
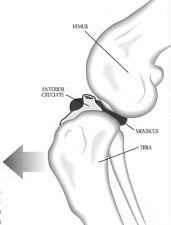
The biomechanics of injury to the anterior cruciate ligament coincide with the functions
of the ligament, which acts as a constraint against one bone (the tibia) moving forward
on the other (the femur). See Fig. 2. The most common mechanism for anterior cruciate rupture comes with sudden rotation of the stifle when the joint is in flexion (i.e. a sudden right turn on the weight-bearing right rear pivot limb). The ligament also ruptures if the knee is hit from the front (as when a football player is hit from the front or when a dog steps in a hole and catches its foot or when he/she falls forward when jumping). Degenerative changes in the stifle joint from obesity, conformational deformities, such as knocked knees, or bowed legs and patellar luxations, or from repeated minor stresses can result in progressive deterioration of the cruciate ligament. When the anterior cruciate ligament ruptures, the compensatory stress placed upon the opposite rear limb may predispose it to ligament rupture. This places critical importance on weight reduction and immediate repair of the damaged leg to minimize the risk to the unaffected limb. SYMPTOMSThe clinical signs of anterior cruciate rupture can vary depending on the extent and chronicity of the injury. Animals with an acute rupture present with a non weight-bearing lameness, joint effusion, palpable pain in the stifle, and joint instability. Those with more chronic injuries generally exhibit an intermittent weight-bearing lameness, muscle atrophy, thickening of the joint capsule with palpable bone spurs present, and joint instability with a frequent "meniscal click" associated with a torn medial meniscus.
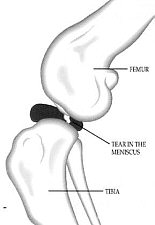
Although the exact purpose of the meniscii is still unclear, they have been described
as elastic, movable washers which aid in the lubrication of the joint and also act as
shock absorbers. The most common meniscal injury occurs in the medial meniscus and is
associated with rupture of the anterior cruciate ligament. In some cases, the meniscus
is crushed between the femur and the tibia. In others, the meniscus may undergo a
longitudinal tear. With this type of lesion, the meniscus may fold on itself during the
abnormal sliding motion of the unstable joint. This type of lesion frequently exhibits
a clicking or snapping sound as the meniscus unfolds. Fig. 3. TREATMENT
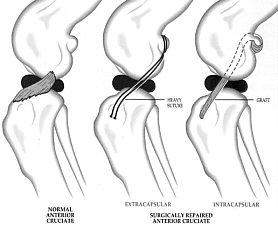
Surgical stabilization of the stifle is recommended for all anterior cruciate ruptures.
Surgical techniques can be divided into extracapsular or intracapsular. The extracapsular
techniques alter the tissues outside the joint to tighten and stabilize the knee. They
include heavy sutures placed outside of, but next to the joint (i.e. modified Flo
imbrication) and the manipulation of ligaments adjacent to, but not inside of, the
joint to stabilize the knee (fibular head transposition). Intracapsular techniques
generally utilize a graft from an adjacent tissue in the knee to replace the anterior
cruciate ligament and are located within the joint capsule. In either case, any damaged
portion of the meniscus and all remnants of the ruptured cruciate ligament are removed
or repaired at the time of corrective cruciate surgery. See Fig. 4. POSTOPERATIVE CAREPostoperative care is critical to long term success. The most crucial element is confinement to a small area. After surgery the knee is bandaged in a stable, walking configuration for one to two weeks. After that time the bandage and sutures are removed and passive physical therapy is started at home. This physical therapy requires only a few minutes three to four times daily. Swimming therapy and short walks, gradually increasing in length over six to eight weeks, will be started several weeks after surgery. Again, complete confinement to a small room, pen or cage when not working on physical therapy is mandatory. Avoid slick floors, jumping, running, stair climbing, and all acrobatics until recovery is complete. |
|