|
|
|
(Kneecap Luxation) (Permission to reprint granted by The Southern California Surgical Group. This article is one of a series of pamphlets produced by this group.).
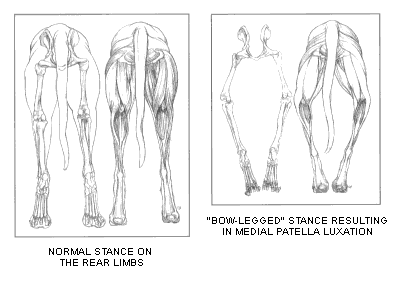
Medial patella luxation, or kneecap luxation, may be congenital (present at birth) or acquired. The congenital form is most common in the toy and miniature breeds such as the Miniature Poodle, Yorkshire Terrier, Toy Poodle, Chihuahua, Pomerianian, and Pekingese, and may occur simultaneously with other pelvic limb deformities. While the definitive sequence of events which leads to or allows these deformities has not yet been established, the age at which the syndrome occurs does play an important role in the severity of the degenerative changes in the joint. When patellar luxations are present early in life, the major
muscle groups of the thigh pull toward the inside of the leg, putting abnormal
pressure on the knee joint cartilage. The result is a bowlegged stance
and an abnormal pull on the patella (Fig. 1). When the patella is in its normal position, its cartilage
surface glides smoothly and painlessly along the cartilage surface of the
trochlear groove with little or not discomfort. As the patella "pops
out" of its groove these cartilage surfaces improperly rub each other. The
animal may cry and try to straighten (extend) the leg to "pop it back
in" or may hold the limb up until muscle relaxation allows the kneecap to
reposition itself. This resembles an intermittent lameness. There is little or
no discomfort until the cartilage is effectively "rubbed off" or
eroded to a point where bone touches bone. From this point on, each time the
patella "pops out" into its abnormal, luxated position it will cause
pain. This explains why many individuals have no clinical lameness until they
reach adulthood. Often progressive cartilage wear creates an acutely painful
condition. Because there is great individual variation in the pathologic deformities seen, a graded classification of medial patellar luxation (Putnam 1968) has been formulated as a basis for recommending which type of surgical repair is most appropriate for each individual. In the following description each classification is addressed. GRADE I The anatomic alignment of the stifle is normal with the patella luxating only when pushed out of socket. GRADE II The patella luxates upon flexion of the joint and remains luxated until returned by manual pressure. GRADE III The patella is permanently dislocated but can be reduced manually with the limb extended. GRADE IV The patella is permanently dislocated and cannot be manually reduced.
POST-OPERATIVE CARE After surgery is completed, the affected leg(s) will be bandaged for approximately 3 to 7 days. Passive physical therapy is begun immediately after bandage removed to work out the stiffness and reestablish a normal range of motion in the joint. During the next 3 to 4 weeks, light walking around the house or supervised short walks outside for eliminating must be strictly controlled (non-acrobatic activity) until a progressive building of muscular support and stamina leads to unrestricted normal function. TREATMENT The procedures for repair of medial patella luxation deal with repositioning and stabilizing the kneecap in the patellar groove of the femur. Depending on the severity of the deformities, the techniques may be as simple as soft tissue reconstruction or as complicated as multiple corrective osteotomies (straightening the bone). The most commonly accepted surgical procedures include ...
|
 Therefore, the statement
"patellar luxation is an anatomic malformation not merely of the knee but
of the entire pelvic limb" ... accurately describes the complexity of a
seemingly simple luxation. Thus, a number of anatomic pelvic limb deformities
can lead to or result from the structural manifestation of medial patellar
luxation. These included bowed legs, coxofemoral (hip) joint abnormalities, and
outward rotation of the limb.
Therefore, the statement
"patellar luxation is an anatomic malformation not merely of the knee but
of the entire pelvic limb" ... accurately describes the complexity of a
seemingly simple luxation. Thus, a number of anatomic pelvic limb deformities
can lead to or result from the structural manifestation of medial patellar
luxation. These included bowed legs, coxofemoral (hip) joint abnormalities, and
outward rotation of the limb.